Table of Contents
- What Are the Long-Term Side Effects of SSRIs No One Talks About?
- Why Do SSRIs Make You Feel Numb Emotionally?
- Do SSRIs Cause Weight Gain in Everyone?
- Are SSRI Withdrawal Symptoms Dangerous?
- Post-SSRI Syndrome (PSSD): The Lingering Effects After Stopping
- How to Talk to Your Doctor Without Being Dismissed
- SSRI Use During Pregnancy: What Women Aren’t Being Told
- What the Research Suggests (Without Medical Advice)
- The Cultural Shame Around Psychiatric Treatment in the U.S.
- When SSRIs Are Life-Saving—And How to Know If It’s Still Working
- State-by-State: SSRI Use, Access, and Patient Trends in the U.S.
- FAQs
- About the Author
What Are the Long-Term Side Effects of SSRIs No One Talks About?
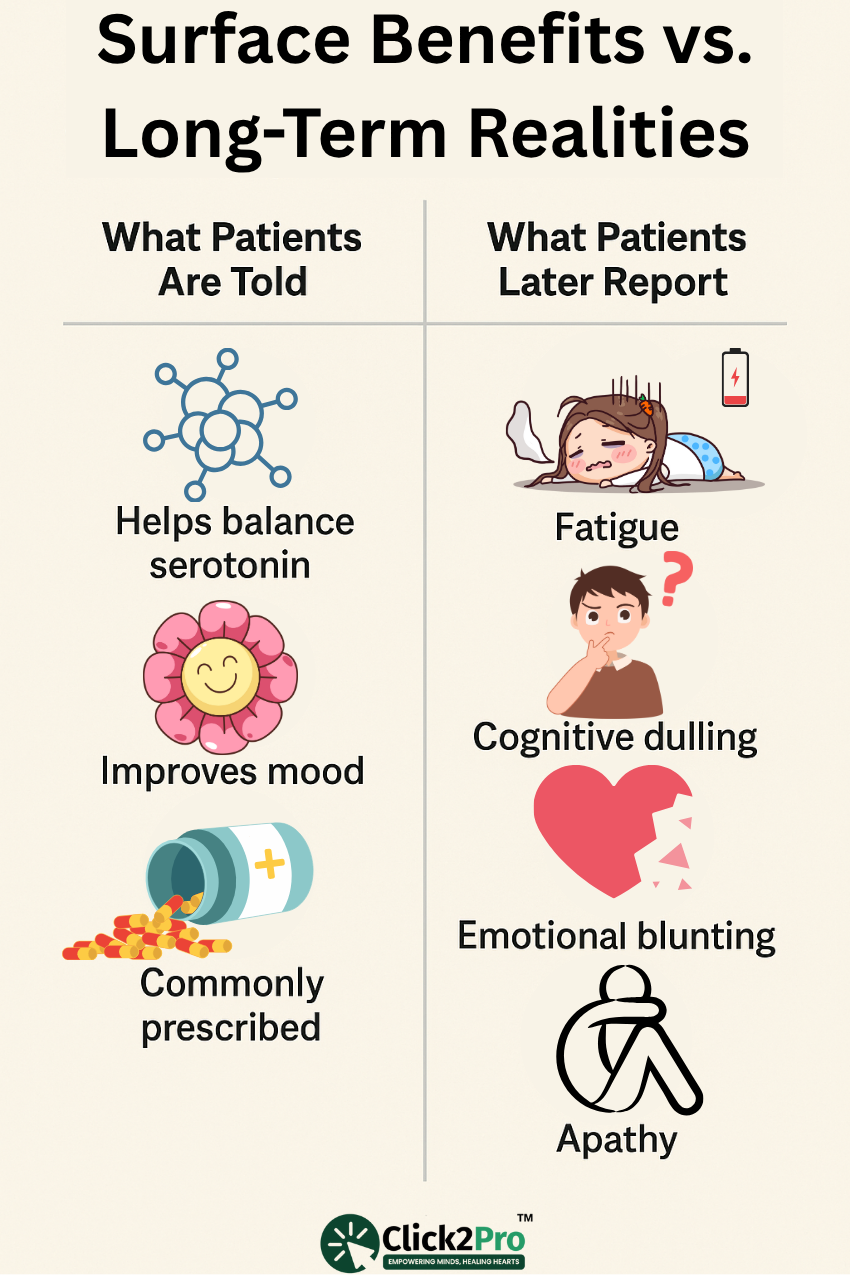
It’s easy to find surface-level information about SSRIs—how they help balance serotonin, how they can ease symptoms of anxiety and depression, and how commonly they’re prescribed in the U.S. But what’s not as widely discussed, especially in primary care settings or quick psychiatric consults, is how these treatments can quietly affect the body and brain when used over an extended period.
In real-world American clinics, especially in states like Ohio, Arkansas, and Nevada where psychiatric follow-up care is often limited, many people remain on SSRIs for years without regular reviews. Prescriptions are refilled routinely, often without a clear discussion about whether the benefits still outweigh the side effects—or if the overall plan should be reevaluated altogether.
People report an array of long-term effects that aren’t typically captured in short-term clinical trials. For example, beyond the commonly cited weight gain or sexual side effects, many describe persistent emotional detachment, chronic fatigue, mental fog, and a subtle but growing sense of “losing themselves.” These effects don’t always show up in the first six months. Instead, they creep in—months or even years after consistent use.
One U.S.-based study found that up to 37% of long-term users experienced symptoms of cognitive dulling—describing it as “thinking through molasses.” Another issue is something users call “motivational depletion”—they’re no longer depressed, but they’re not particularly driven either. This has a significant impact on professionals in high-performance roles like software engineers in Austin or marketing managers in Chicago, who rely on clarity and creativity to function.
In addition, gut-brain interactions are another emerging topic. Some long-term users report worsening digestion, bloating, or chronic nausea. These may be tied to serotonin’s critical role in the gastrointestinal system—a fact rarely emphasized in standard consultations.
There’s also a conversation to be had around apathy. Not the full-body sluggishness of depression, but rather a quiet disengagement from previously meaningful experiences. This isn’t just “not feeling sad”—it’s not feeling much at all.
For many, this experience becomes the reason they eventually explore whether continuing is still the right choice. But by the time it’s recognized, some people feel stuck—afraid that making changes or stepping away might bring back the overwhelming emotional pain they were trying so hard to escape in the first place.
Why Do SSRIs Make You Feel Numb Emotionally?
Perhaps one of the most puzzling—and distressing—effects people report is emotional blunting. Individuals often describe it as “feeling flat,” “like I’m underwater,” or “unable to cry even at a funeral.” This isn’t just a small annoyance—it can fundamentally change how someone experiences relationships, joy, grief, or even a sense of identity.
The mechanism behind this is not entirely mysterious. SSRIs increase serotonin availability in the brain, but they also alter how the brain responds to stimuli—both positive and negative. In theory, this helps protect against spirals of negative emotion. But in practice, it sometimes mutes everything.
This flattening effect tends to be more common among long-term users, but it can show up early as well. Some people feel better initially—less anxious, more level—but as time goes on, they notice that while the lows are gone, so are the highs. Passion fades. Humor doesn’t hit the same. A romantic moment that should’ve sparked tears of joy instead feels... distant.
One client I worked with—a 29-year-old kindergarten teacher in Denver—explained it like this:
“I’m not sad anymore. But I also don’t feel the sparkle of life. My kids laugh, and I know I should feel something—but I don’t.”
Her story is far from rare.
Men and women often describe this effect differently. For men, it’s commonly expressed as “zoning out,” or “just not reacting to anything anymore.” For women, it may be mistaken for postpartum depression or burnout—especially among mothers managing both career and childcare. These emotional shifts are frequently overlooked or attributed to other life factors.
What’s especially challenging is that this emotional flattening is not always discussed unless someone asks directly. That leaves many people wondering if what they’re experiencing is part of the healing process or something that needs more attention.
It also impacts relationships. Partners may see the lack of emotional response as distance. Parents might feel they’re struggling to bond with their children. Some individuals even say they feel disconnected from their own identity:
“I’m still me, but muted.”
In an attempt to feel more alive, some people try to stimulate emotion through risk-taking, overworking, or high-adrenaline activities. Others consider making big life changes—moving, leaving relationships, switching jobs—not out of unhappiness, but in hopes of sparking feeling.
Many carry guilt for even questioning their current path, afraid it means they’re being ungrateful for how far they’ve come. It’s a deeply human contradiction: being thankful for emotional stability, but quietly grieving the depth and intensity that once came with the struggle.

Do SSRIs Cause Weight Gain in Everyone?
No, not everyone gains weight while taking SSRIs—but enough people do that it’s become one of the most common reasons people in the U.S. begin questioning whether they should continue with their current treatment.
Weight gain isn’t just a cosmetic concern. For many individuals—especially women in professions where appearance impacts confidence or credibility, like nurses, fitness trainers, or real estate agents—it can take a serious toll on self-esteem and performance at work. Men, too, report frustration, particularly those in physically demanding roles like construction, firefighting, or logistics.
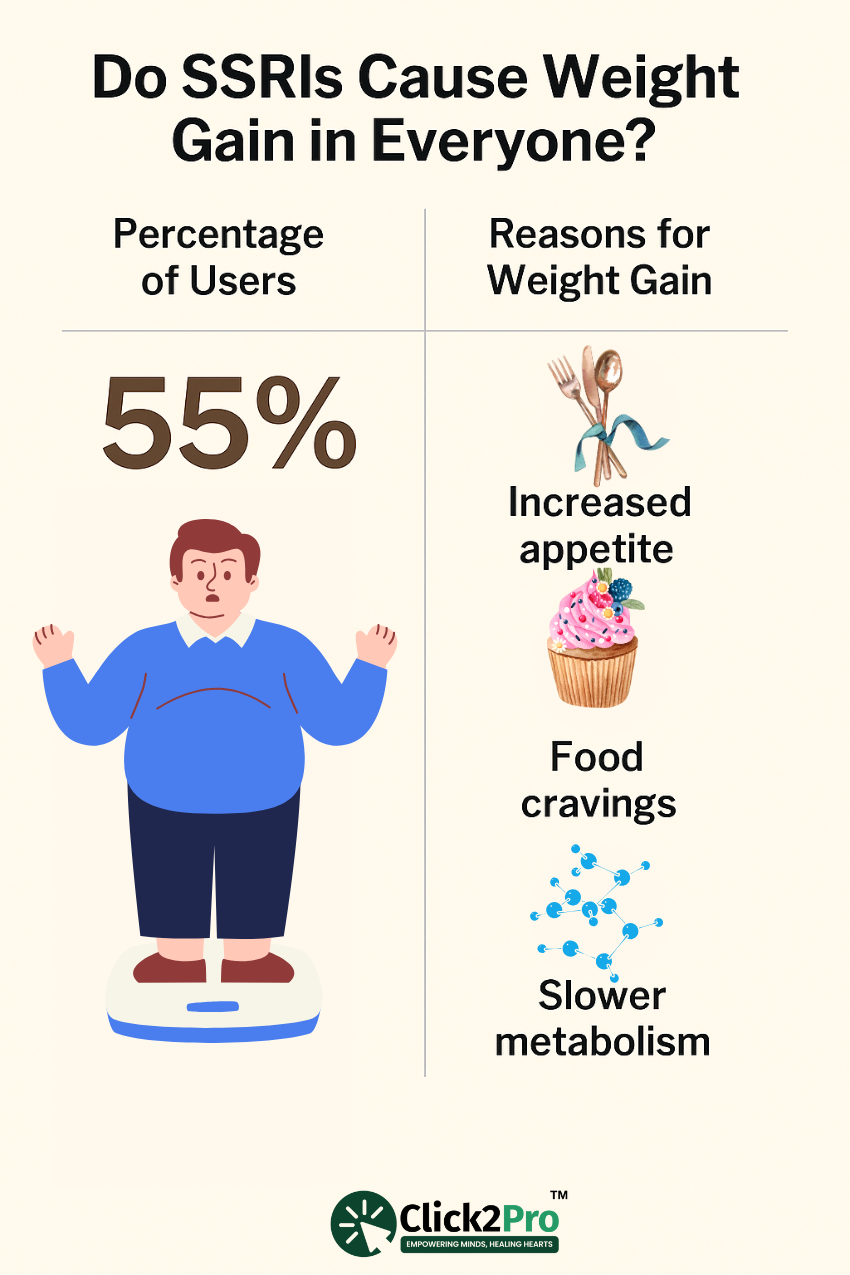
Some people start noticing changes within the first three months. For others, it’s more gradual—three pounds here, five pounds there—until it adds up. A large-scale study of over 22,000 individuals across U.S. health systems revealed that up to 55% gained more than 10 pounds within one year, with certain SSRI options like paroxetine and sertraline associated with the highest average increases.
But why does this happen?
Science points to several possible explanations. SSRIs can influence serotonin, which helps regulate hunger and satiety signals. Some people report new cravings—particularly for carbs and sweets—even if they never had them before. Others describe emotional eating returning once their anxiety eases, replacing one coping habit with another.
There’s also metabolism. Some researchers believe that SSRIs may lower the body’s basal metabolic rate (BMR), meaning fewer calories are burned at rest. Combined with increased appetite, this shift can easily lead to weight gain over time.
Unfortunately, this concern is often dismissed. Some providers brush it off or attribute it to lifestyle habits. A 42-year-old woman from Tallahassee shared that she gained 18 pounds in 9 months, only to be told it was “probably menopause”—despite having no other hormonal changes.
Then there’s the emotional weight of the issue. Many individuals hesitate to bring it up, worried they’ll be seen as superficial—or worse, ungrateful for the stability they’ve found. But when weight gain becomes distressing, people sometimes skip doses, reduce their intake on their own, or stop altogether without support, which can lead to new challenges, both physical and emotional.
The truth is, not all SSRIs have the same effect. While some are associated with more significant weight changes, others seem to have little to no impact—and in a few cases, appetite may even decrease. Still, these patterns vary greatly from person to person.
At its core, this isn’t about vanity. It’s about feeling like yourself again. And anyone navigating these changes deserves to discuss them openly—without shame, without dismissal, and with genuine support.
Are SSRI Withdrawal Symptoms Dangerous?
One of the most misunderstood aspects of SSRI use is what happens when someone decides it’s time to stop.
First, let’s be clear: SSRIs are not chemically addictive like opioids or benzodiazepines. There’s no craving, no euphoric high. But even without those traits, stopping abruptly or tapering too quickly can lead to powerful, sometimes frightening symptoms—a condition often referred to as SSRI discontinuation syndrome.
People often describe these symptoms as “brain zaps,” sudden electric shock sensations in the head. Others experience dizziness, nausea, insomnia, intense irritability, or a return of panic—sometimes even if those symptoms weren’t part of the original condition.
A software developer in Seattle shared her experience after tapering off sertraline over two weeks:
“It felt like the ground was moving under my feet. I couldn’t think straight. I was crying in meetings and getting random shocks in my neck and jaw.”
Her provider later confirmed the process had been too fast.
These stories aren’t rare. A 2022 mental health survey in the U.S. found that 1 in 4 people who stopped using SSRIs experienced moderate to severe withdrawal symptoms, lasting from a few days to several weeks. The risk increases with longer usage and with certain types—especially those with shorter half-lives like paroxetine, which leaves the body faster and tends to cause more intense symptoms.
Unfortunately, many people say their concerns are dismissed. These effects are sometimes misdiagnosed as relapse, leading individuals to believe they have no choice but to continue indefinitely—even if they’re no longer struggling with their original condition.
Some try to manage the process alone, using pill-splitting or taking doses every other day. But without guidance, this often leads to a rollercoaster of symptoms that can disrupt sleep, work, and relationships.
So, are withdrawal symptoms dangerous? They can be—especially if they contribute to risky decisions, emotional distress, or job-related consequences. While not typically life-threatening, these effects are real, and they deserve more recognition in everyday mental health care across the U.S.
The safest way forward is a slow, strategic approach—guided by someone experienced with these challenges. Some people reduce their dosage by as little as 5–10% every few weeks. The process might take months—or even longer—but this gentler pace can make a huge difference in how the body and mind adjust.
Ultimately, education is what matters most. When people know what to expect, they’re less likely to panic. They can plan, ask the right questions, and move through the process with more clarity and confidence.
Withdrawal isn’t failure. It’s a transition—and with the right support, it’s absolutely possible.
Post-SSRI Syndrome (PSSD): The Lingering Effects After Stopping
For many, stopping an SSRI marks the end of a difficult chapter—but for others, it signals the start of a new and often misunderstood struggle: Post-SSRI Sexual Dysfunction (PSSD). This condition, still under-recognized in U.S. psychiatric circles, refers to persistent sexual side effects that continue long after the use of SSRIs has ended—sometimes for months, even years.
While it’s well-known that SSRIs can affect sexual function during use—such as lowering libido, delaying orgasm, or causing genital numbness—what's rarely discussed is that these issues may persist long after use has stopped. In some cases, symptoms even begin only after the treatment ends.
What Does PSSD Feel Like?
Patients report:
-
Loss of genital sensation (often described as "numbness" or “no connection” between mind and body)
-
Absence of arousal even in emotionally intimate or physically stimulating scenarios
-
Inability to orgasm, or severely delayed orgasm
-
Low or nonexistent libido despite no psychological symptoms of depression
A 2024 U.S. survey conducted among online mental health forums found that nearly 11% of patients who discontinued SSRIs still reported sexual dysfunction 6–12 months later, with no prior sexual health issues.
This isn't just about sex—it impacts self-esteem, relationships, identity, and mental health recovery. Patients report feeling "disconnected from their bodies," and some even question if they’ll ever return to who they were before treatment.
Real Stories from U.S. Patients
“It was like someone turned off a switch. I stopped Zoloft a year ago, and I still feel nothing. I’ve been with my partner for five years—we’re close, we love each other—but that spark is just gone.”
— Jonathan, 36, Cleveland, OH
“I never had issues before taking Lexapro. Three months after stopping, I noticed I still had no drive. I thought it was depression, but I felt happy otherwise. It’s just my body won’t cooperate.”
— Renee, 28, Fresno, CA
Why Is PSSD Not Diagnosed More Often?
There are a few reasons:
-
Lack of awareness: Many U.S. psychiatrists don’t recognize PSSD as a distinct syndrome
-
Shame or embarrassment: Patients often don’t report sexual dysfunction unless directly asked
-
Misdiagnosis: PSSD is often mistaken for depression relapse, low testosterone, or relationship stress
The U.S. FDA does not currently list PSSD as an official risk on most SSRI drug labels, though advocacy groups and researchers have pushed for this to change.
So What Can Be Done?
There is no definitive treatment for PSSD yet, but some patients explore:
-
Pelvic therapy or somatic-focused psychotherapy
-
Mindfulness-based sexual health interventions
-
Tapering protocols that minimize serotonergic disruption (under psychiatric care)
-
Ongoing research trials into post-SSRI neuroadaptation
Still, the first step is naming it—giving patients validation that what they’re experiencing is not imaginary or shameful.
How to Talk to Your Doctor Without Being Dismissed
Many Americans don’t just struggle with side effects—they struggle with being believed. In clinics from Georgia to Minnesota, people often report that their concerns about SSRIs are minimized. They’re told, “That’s just your depression talking,” or “It’s better than how you felt before,” or worse, “You’re imagining it.”
This dismissal doesn’t usually come from cruelty. More often, it stems from time pressure—many psychiatric appointments in the U.S. are limited to 15 minutes—or from a lack of awareness around subtle or delayed effects. Still, the result is the same: the person leaves feeling unheard and unsure of what to do next.
So how can you talk to your doctor in a way that gets results?
Start by being specific. Instead of saying, “I don’t feel like myself,” try something more direct:
“Since starting this, I can’t cry, even when I feel like I should. I’ve also stopped laughing or enjoying things I used to love.”
This helps your doctor tell the difference between lingering emotional symptoms and new side effects.
Another helpful step is to keep a symptom journal for 2–4 weeks. Track any emotional shifts, appetite changes, memory lapses, or physical concerns like fatigue, restlessness, or nausea. Bringing this log to your appointment makes the conversation grounded in facts—not just feelings.
It can also help to bring a trusted friend or family member with you. In states like California and Massachusetts, it's common for support people to join mental health consults. Their presence shows you’re taking this seriously and offers an extra perspective on how things have changed.
Here’s a simple script to open the conversation:
“I’m thankful for the stability I’ve gained. But recently, I’ve been noticing some changes that are affecting how I feel day to day. I want to explore what might be causing them—and talk through what options we have.”
Notice the tone—collaborative, not confrontational. Most doctors respond more openly when they don’t feel blamed or challenged.
If your concerns are still brushed off, don’t give up. Consider getting a second opinion. Telehealth has made it easier than ever to connect with providers in different states—especially those trained in trauma-informed care or experienced with SSRI-related side effects.
The key takeaway: advocating for your mental health isn’t being difficult—it’s being responsible. You deserve to feel fully heard and supported, not just “functional.”
Many individuals now explore online counselling sessions as a safer, more flexible way to discuss side effects they once felt too ashamed to mention in person—especially in states where in-person psychiatric care remains limited.
SSRI Use During Pregnancy: What Women Aren’t Being Told
When a woman in the U.S. finds out she’s pregnant while using an SSRI, she often faces a flood of mixed emotions—and very few clear answers. The internet is full of conflicting advice, and even doctors may offer different guidance depending on location, training, or available resources. For many expecting mothers, the question isn’t just “Is this safe?” It’s “Why didn’t anyone warn me how complicated this would be?”
The Silent Anxiety of Pregnant Women on SSRIs
Across the country—from Los Angeles to Dallas to Buffalo—pregnant women taking SSRIs like Zoloft, Lexapro, or Prozac often share the same fears:
-
Will this affect my baby?
-
Will I feel worse if I stop?
-
What are the risks of continuing?
-
Why wasn’t this explained when I started?
Many report feeling rushed to make a decision—often without the full picture. One Chicago-based therapist shared that half of her prenatal clients felt they were “left alone to Google the answers” after their OB-GYNs referred them to psychiatry... only to discover wait times of six weeks or more.
In states like Texas, OB-GYNs tend to be cautious, avoiding certain prescriptions due to liability concerns. Meanwhile, in California, where integrated care systems are more common, pregnant women may have access to perinatal psychiatrists who can offer more thorough evaluations. Still, most women across the U.S. don’t have access to specialized care, and important guidance often depends on their zip code and insurance provider.
The result? Expecting mothers are left to navigate complex emotional and medical decisions without a clear support system—often juggling risks to their mental health with concern for their baby’s well-being, all while managing judgment from others.
What the Research Suggests (Without Medical Advice)
The research on SSRI use during pregnancy is nuanced—and interpreting that data can be overwhelming for expecting parents.
Some studies suggest a slightly increased risk of preterm birth, neonatal adaptation syndrome (NAS), or low birth weight, especially when SSRIs are used during the third trimester.
At the same time, untreated maternal depression also presents real risks. These can include early delivery, complications after birth, and long-term emotional or physical health challenges for both parent and child.
Among the available options, sertraline is frequently mentioned by U.S. mental health professionals as one of the most extensively studied for use during pregnancy. However, being well-studied does not mean being entirely free of risk.
What often goes unspoken is this: Every case is personal. For some, continuing treatment during pregnancy supports both emotional and physical stability. For others, it might make sense to reduce dosage, change the approach, or focus on therapeutic support. The decision depends not just on medical facts but on personal history, current needs, and access to care.
The Missing Support Conversation
Beyond science lies a heavy emotional burden. Many women carry guilt for using SSRIs during pregnancy—even when it's helping them remain stable and engaged in their lives. This guilt is often magnified by online opinions, social pressure, or comments from well-meaning family members.
A schoolteacher from North Carolina shared:
“My OB told me Zoloft was fine, but my mom said, ‘You’re going to harm your baby.’ I was caught between fear, shame, and total confusion. I ended up cutting my dose without telling my doctor—and three weeks later, I could barely get out of bed.”
This type of experience is far too common—especially in areas where mental health is not integrated into prenatal care conversations.
What Should Be Happening Instead?
Here’s what women navigating pregnancy and emotional wellness deserve—but too often don’t receive—in the U.S.:
-
A nonjudgmental, collaborative conversation about risks, benefits, and alternatives
-
Referrals to perinatal mental health specialists, not just general practitioners
-
Validation that emotional well-being is a vital part of prenatal health
-
Support systems that recognize how deeply connected maternal and infant health really are
Maternal health advocates continue pushing for improved mental health screening during pregnancy, as well as more accessible care through telehealth platforms like Click2Pro. This is especially urgent in under-resourced states like Mississippi, West Virginia, and Idaho, where prenatal psychiatric support is scarce.
SSRIs and Breastfeeding: A Separate Yet Connected Concern
For many new mothers, the fear doesn’t end after birth. Those who choose to breastfeed often face another layer of anxiety.
Some research shows that small traces of SSRIs can pass into breast milk, though the levels—and their clinical relevance—vary.
Among commonly discussed options, sertraline is often viewed as the most breastfeeding-compatible by U.S. lactation consultants. But even then, concerns remain. Mothers worry: Will this make my baby drowsy, overly alert, or emotionally affected?
As a result, some mothers stop breastfeeding earlier than planned—or avoid emotional support treatments altogether—sacrificing their well-being out of fear, not information.
The Cultural Shame Around Psychiatric Treatment in the U.S.
In the U.S., taking antidepressants is no longer the taboo it once was—but the shame hasn’t entirely disappeared. It’s simply evolved. Instead of hearing “You’re crazy,” people often face more subtle forms of judgment:
“You’re weak.”
“You just need to exercise and pray.”
“You’re not trying hard enough.”
For many, this quiet judgment creates an internal tug-of-war. They credit their stability to the support they received—but still feel hesitant to talk about it. This conflict is especially common in tight-knit communities, religious spaces, and among professionals in caregiving roles like teachers, pastors, or nurses.
One woman in rural Mississippi shared that she kept her SSRI use a secret from her church group for two years:
“They talk about how ‘God heals all wounds’—and I believe that. But God also made scientists. Why should I feel ashamed for needing both?”
Among Black, Latino, and Asian-American communities, the stigma often runs deeper. Mental health is still commonly viewed as something to be handled privately—or not discussed at all. Studies show these groups are significantly less likely to seek emotional support and more likely to stop treatment early due to cultural or family pressure.
Men are also deeply affected. In places like Texas and Pennsylvania, where masculinity is often tied to stoicism and self-reliance, many men avoid therapy or hide their routines out of fear of appearing “soft.” One construction worker in Scranton said:
“I keep my meds in a vitamin bottle. No one needs to know.”
Even celebrities aren’t immune. Public figures like Dwayne “The Rock” Johnson and Selena Gomez have spoken openly about their mental health journeys—and the backlash they’ve received for being “too open” or “too vulnerable.”
But here’s the truth: taking care of your mental health is a sign of strength—not weakness. In fact, facing stigma head-on while prioritizing your emotional well-being is one of the most courageous things a person can do.
There’s hope, though. The stigma is shifting.
Younger generations—especially Gen Z—are rewriting the narrative. They’re talking openly about therapy, emotional regulation, and self-awareness. Platforms like TikTok, Instagram, and mental health podcasts are normalizing what used to be whispered in secret.
Across the U.S., more people are saying, “I take care of my mental health—and I’m not ashamed.”
Still, there’s more work to do. Every voice that speaks up creates space for others. Every honest conversation chips away at decades of silence. And every professional who listens—truly listens—helps rebuild trust where it’s been broken for far too long.
When SSRIs Are Life-Saving—And How to Know If It’s Still Working
For many patients, SSRIs are more than just a treatment plan—they’re a lifeline. They've helped countless Americans climb out of depression, sleep through the night again, and reclaim their daily functioning. The success stories are real. A college student in Oregon who once contemplated suicide now attends therapy, manages her coursework, and credits this support for helping her stay afloat during her darkest semester.
But just because something helped you once doesn’t mean it’s the right fit forever.
One of the most overlooked aspects of long-term SSRI use in the U.S. is the lack of re-evaluation. It’s common for individuals to continue on the same course for years without reassessing whether it’s still effective—or even necessary.
Is It Still Working? How to Spot the Signs
Here are subtle red flags that may suggest it’s time to take a closer look:
-
You feel emotionally flat or disconnected even as life circumstances improve
-
Your major symptoms have eased, but you no longer feel excited about anything
-
Day-to-day drawbacks now seem more impactful than the original benefits
-
Emotional or physical symptoms are returning despite consistency in use
In some cases, the brain adapts over time. What once worked may become less impactful due to tolerance. In others, life circumstances have shifted—maybe you’ve started therapy, built strong social connections, or changed environments—making the old support structure less relevant.
You Don’t Have to Be in Crisis to Reassess
Improvement isn’t binary. Just because you’re not in bed all day doesn’t mean you’re thriving. Many people live in a state of quiet disconnection—handling responsibilities while feeling dulled, detached, or emotionally neutral.
That doesn’t have to be your ceiling.
Feeling better doesn’t mean giving up curiosity about how you could feel even more engaged, motivated, or present.
When Should You Reevaluate?
Experts recommend reviewing your care approach every 6–12 months, especially if you’ve followed the same path for more than two years. This doesn’t mean you need to stop—it simply gives you the chance to reflect and adjust.
That adjustment might look like:
-
Tweaking your approach or adding therapy
-
Shifting focus to a different type of support
-
Slowly stepping back, if that feels aligned with your progress
You won’t know what’s possible unless you ask the right questions—and feel safe enough to explore the answers.
Support Should Grow With You
Mental health is not static—it evolves. What you needed three years ago may be different than what you need today. The right tools should support that growth, not stall it.
It’s okay to ask: “Is this still serving me?”
And if the answer isn’t a clear yes, it might be time to explore what else is out there—without shame, fear, or pressure.
State-by-State: SSRI Use, Access, and Patient Trends in the U.S.
SSRIs are prescribed across all 50 states, but how Americans access and experience these treatments varies significantly depending on geography, available resources, and healthcare systems.
Which states see the highest usage rates?
According to CDC data, West Virginia, Maine, and Kentucky lead the nation. These states also rank high in depression and anxiety rates, often tied to economic hardship and a lack of mental health infrastructure. In these areas, primary care physicians—not mental health specialists—issue more than 75% of all prescriptions related to mood and emotional stabilization.
Contrast that with California, New York, and Massachusetts, where large urban centers provide broader access to therapy networks, academic hospital systems, and diversified treatment plans. Yet even in these states, rural regions face serious provider shortages, with many counties lacking access to a single licensed therapist or psychiatrist.
The Telehealth Surge and Its Impact
The digital divide has created both challenges and solutions. Since 2020, states like Texas, Florida, and Washington have seen a rapid expansion in teletherapy and virtual psychiatry. Platforms like Click2Pro have made it possible for patients in remote areas to connect with professionals across state lines—filling gaps where local options fall short.
Insurance: The Hidden Gatekeeper
Coverage policies shape access more than most people realize. In states like Louisiana and Alabama, Medicaid recipients often face long wait times or limited treatment options. In contrast, residents in Colorado or Illinois with private insurance tend to have better access—but may still face high co-pays, referral red tape, or plan exclusions that complicate care.
Teen Trends and Post-Pandemic Shifts
A concerning trend is emerging among adolescents. In Utah and Arizona, mental health professionals report a sharp increase in emotional support plans for teens aged 13 to 17, especially after 2020. School counselors note spikes in anxiety, academic pressure, and social detachment. Early intervention has become a growing area of focus in school districts trying to reduce long-term emotional fallout.
Cultural Gaps in Access and Trust
Some communities remain significantly underserved—not just due to logistics, but cultural disconnect. On Native American reservations, or among undocumented immigrants, the issue isn’t just about reaching a therapist—it’s about trust, language, and feeling seen. Many avoid seeking help altogether due to stigma or fear of institutional barriers.
FAQs
-
What are the long-term side effects of SSRIs no one talks about?
Long-term SSRI use can quietly lead to side effects like emotional numbness, brain fog, fatigue, and lack of motivation. Some users also report sexual dysfunction that continues even after stopping. These changes often develop slowly, making them harder to recognize.
-
Why do SSRIs make you feel numb emotionally?
SSRIs boost serotonin to stabilize mood, but in some people, this leads to emotional blunting. Highs and lows become less intense, and daily experiences may feel flat. Over time, it can feel like losing access to your own emotions—a common concern for long-term users.
-
Do SSRIs cause weight gain in everyone?
No, but many users do gain weight—especially those using certain types. The cause often includes increased appetite, carbohydrate cravings, and possible slower metabolism. This can affect energy levels and body confidence, particularly in professions where appearance matters.
-
Are SSRI withdrawal symptoms dangerous?
Withdrawal symptoms aren’t usually life-threatening, but they can be intensely uncomfortable. People report brain zaps, dizziness, insomnia, and emotional spikes. Tapering slowly with the help of a professional reduces risks and gives your body time to adjust.
-
Can you stay on SSRIs forever?
Some people remain on SSRIs for years, especially when symptoms are long-term. But ongoing check-ins are crucial. What helped at one stage of life might not be necessary—or effective—down the road. Regular reassessment ensures continued benefit without unwanted effects.
-
How do I know if my SSRI is still working?
If you feel numb, emotionally flat, or symptoms have crept back in, it may be time for a review. A lack of joy or growing side effects could mean your current plan needs to shift. Mental health support should evolve with your life—not keep you stuck.
About the Author
Dr. Tanya Arora is a licensed clinical psychologist with over 15 years of experience supporting individuals across the U.S. through life’s challenges—from anxiety and depression to life transitions, relationships, and parenting concerns. A proud member of the American Psychological Association, she holds a Doctorate in Clinical Psychology and brings a human-first, evidence-based approach to her work.
At Click2Pro, Dr. Arora specializes in integrative mental health care, working with diverse clients across cultures, ages, and backgrounds. She’s particularly passionate about helping people find their voice—whether that means navigating medication decisions, building emotional resilience, or rediscovering passion after feeling numb.
Dr. Arora has published articles in professional journals on mindful care, patient advocacy, and bridging gaps in mental health access. Her work has been featured in national publications and podcasts, where she advocates for transparent, empathetic care and dismantling stigma around psychiatric support.
When she isn’t working with clients, Dr. Arora develops training content for mental health professionals and leads community workshops focused on emotional wellness, trauma-informed support, and navigating life transitions with integrity and courage.