Table of Contents
- Why “Overcare” Is the New Hidden Abuse
- Spotting the Red Flags: What U.S. Pediatricians and Teachers Miss
- Psychological Profile of the Perpetrator: It’s Not Just ‘Crazy Moms’
- The Silent Suffering of the Child: Trauma, Identity Confusion & Mental Health
- When the System Fails: CPS, Hospitals & Legal Loopholes
- Digital Munchausen: When MBP Goes Online
- Therapy and Recovery for Victims: Healing After Coercion
- Can You Report Suspicion of Munchausen by Proxy? Yes—Here’s How
- Conclusion
- FAQs
- About the Author
Why “Overcare” Is the New Hidden Abuse
In homes that look picture-perfect, hidden forms of abuse can take root quietly. One of the most dangerous is Munchausen by Proxy (MBP)—a psychological manipulation where a caregiver, often a parent, fabricates or induces illness in someone under their care, typically a child. This is not a mental illness in the victim, but a deliberate strategy of deception and coercion by the abuser. And in the United States, this tactic often hides in plain sight under the veil of “exceptional caregiving.”
Many Americans are taught to admire self-sacrificing mothers or tireless caregivers. In suburban Illinois or affluent parts of Texas, neighbors may see a mom taking her child to the ER repeatedly and assume she’s devoted. But what they may not see is the emotional and sometimes physical harm behind that performance.
While the term “Munchausen by Proxy” might sound clinical or outdated, the damage it causes is alarmingly real. The American Academy of Pediatrics and child protection agencies now classify it as a form of medical child abuse—but it often goes unrecognized until serious harm has occurred. Unlike other forms of abuse that may leave bruises, MBP leaves emotional scars, confused identities, and trauma that can take decades to uncover.
According to recent child welfare reviews, fewer than 15% of MBP cases in the U.S. are detected early. This is partly because the abuse presents itself as caregiving. The child may seem constantly ill, in need of procedures, medications, or doctor visits. But when physicians begin to find no medical explanation, and yet the caregiver pushes for more tests or insists something is wrong, a deeper issue may be at play.
What makes this abuse especially difficult to detect is that the child is often groomed to participate in the deception. In some situations, they are taught to believe they are sick. In others, their symptoms are actually induced through medication, food restriction, or other harmful means. The caregiver—frequently the mother—positions herself as the hero, the advocate, the one who "fights for answers." This becomes a social identity reinforced by community support and even admiration.
Some survivors have shared that they spent their entire childhood believing they were terminally ill, only to discover in adulthood that they had been manipulated. The betrayal is profound. One young adult from Colorado recounted that his mother used feeding tubes and oxygen tanks unnecessarily, keeping him dependent for over a decade. He didn’t realize the truth until he entered college and lived independently for the first time. “My whole identity had been wrapped up in being sick,” he said. “When I wasn’t sick anymore, I didn’t know who I was.”
This isn’t just emotional abuse—it is identity theft. The child’s sense of reality, bodily autonomy, and trust in caregivers is eroded. This is why MBP survivors often struggle later with depression, anxiety, trust issues, and even dissociation. For many, therapy becomes essential—not just to unpack the trauma but to understand who they are without the label of illness.
In 2024, the U.S. saw a slight increase in reported MBP cases, particularly in urban pediatric centers in California and Florida. Experts believe the numbers are still severely underreported. In truth, most cases only come to light when a third party—such as a school nurse, therapist, or medical professional—starts to notice the pattern and sounds the alarm.

Spotting the Red Flags: What U.S. Pediatricians and Teachers Miss
Despite mandatory reporter laws in all 50 states, many pediatricians, school nurses, and educators still miss the early signs of Munchausen by Proxy. This is not due to negligence—it’s because the abuse is designed to look like love.
In cases of MBP, the caregiver is often charismatic and persuasive. They come armed with binders of medical records, detailed notes, and a list of previous diagnoses—some real, some fabricated. Pediatricians may feel overwhelmed by the caregiver’s advocacy and assume they are dealing with a particularly complicated medical case. The child, coached by the caregiver, may recite symptoms or express fears that sound genuine. And because doctors are trained to trust their patients and families, they may overlook the subtle inconsistencies.
One red flag that often gets missed is medical inconsistency. The child may show symptoms only when the caregiver is present. Their test results may not align with their complaints. A pediatrician in New York reported a case where a 9-year-old girl had recurring seizures—until hospital staff isolated her from her mother. The episodes stopped completely. That’s when suspicion turned into investigation.
Schools, too, are crucial environments where signs of MBP can surface—but often don’t. Teachers may notice a child frequently missing class for “medical issues,” or being discouraged from participating in activities like gym or field trips. In states like Michigan and Pennsylvania, school counselors have received training to detect patterns of fabricated illness. But even then, it's hard to differentiate between genuine chronic health conditions and carefully manufactured ones.
Another warning sign is a child who seems too knowledgeable about medical terms for their age. In a recent case in Arizona, an 8-year-old boy could name all the medications he was taking and described procedures in clinical detail. His teacher found this odd and mentioned it to the school nurse. That small observation initiated a review that uncovered the caregiver's long history of exaggerating and inventing his symptoms.
Unfortunately, many teachers and pediatricians feel ill-equipped to handle suspicions of MBP. They fear false accusations or breaking trust with families. This is why child advocacy centers across the U.S. are working to bridge the gap between suspicion and action. In Texas, for example, some hospitals now have multidisciplinary teams trained in MBP detection—including psychologists, social workers, and forensic pediatricians.
But the burden should not fall only on professionals. Community awareness matters too. Grandparents, neighbors, family friends—anyone who notices a pattern of exaggerated illness claims, conflicting doctor visits, or a child who never seems to “get better”—can help initiate the process of intervention.
The most effective tool remains documentation. School staff and medical providers are encouraged to keep clear notes on discrepancies, missed school days, medical visits, and caregiver interactions. Over time, these records can create the evidence needed for CPS to intervene.
While MBP can occur anywhere, it is more frequently identified in families with access to multiple healthcare providers, a pattern seen in higher-income areas of New Jersey, Connecticut, and California. This is not because wealth causes MBP, but because it allows for more medical “shopping,” multiple doctor visits, and the ability to hide manipulation behind privilege.
Spotting MBP requires both intuition and data. And while pediatricians and teachers play a critical role, training alone isn’t enough. It takes awareness, documentation, and the courage to speak up—especially when the abuse is wrapped in affection.
Psychological Profile of the Perpetrator: It’s Not Just ‘Crazy Moms’
It’s easy—and dangerous—to assume that every case of Munchausen by Proxy involves a “mentally unstable mother.” This assumption not only overlooks the complexity of the disorder but also prevents proper understanding and intervention. The psychological profile of a perpetrator is more nuanced, often wrapped in traits that appear socially acceptable or even admirable on the surface.
Clinically speaking, many caregivers who engage in MBP present with traits commonly associated with narcissistic personality disorder, borderline personality tendencies, or unresolved trauma. But not all of them meet the diagnostic criteria for a mental illness. In fact, many function successfully in society. They may hold jobs, volunteer at their child’s school, or serve on the PTA. The persona they show to the outside world is polished. This is part of the deception.
What motivates such caregivers? Often, it’s not the child’s wellbeing—but their own emotional needs. In many documented U.S. cases, including one in suburban New Jersey and another in Minnesota, perpetrators expressed that being seen as a “strong caregiver” gave them attention, validation, and control. Some even became local celebrities in their communities—raising funds for rare diseases or blogging about their “medical journeys.” But behind closed doors, they were harming their children to maintain this identity.
These behaviors are sometimes rooted in early abandonment or childhood trauma. For example, a psychological review of 38 convicted MBP offenders in the U.S. found that nearly 70% had experienced some form of emotional neglect as children. Their need to be seen, validated, or pitied often grows out of a deep well of unmet emotional needs. But instead of seeking therapy, they turn to controlling someone else’s health as a way to fulfill that void.
It’s also crucial to note that perpetrators are not always women. Although most reported MBP cases involve mothers, there are known instances involving fathers, step-parents, grandparents, and even foster caregivers. In a rare 2022 case from Washington state, a father coached his daughter into pretending she was blind, leading to a prolonged CPS investigation that uncovered years of medical deception.
Perpetrators of MBP are often very persuasive. They can manipulate doctors, divide family members, and even fool law enforcement. This ability to control the narrative makes them particularly dangerous. And because they often use the healthcare system as their stage, their victims—children—become voiceless props in a performance of endless caregiving.
What separates MBP from general overprotectiveness or anxiety is intent. While some parents may genuinely worry excessively about their child’s health, MBP involves deliberate deception. The caregiver knows the child isn’t sick but still insists on medical attention, invasive tests, or dangerous treatments.
Understanding this psychological profile is essential for professionals in the field. It helps separate misguided care from abuse. And for survivors, recognizing that the abuse wasn’t about their health—but about their caregiver’s need for control—can be the beginning of healing.

The Silent Suffering of the Child: Trauma, Identity Confusion & Mental Health
For the child caught in the web of Munchausen by Proxy, the damage is not only physical—it’s deeply psychological. These children grow up believing their bodies are broken, that they’re fragile, or that the world is dangerous. This belief system is often intentionally installed by the caregiver and reinforced with every false diagnosis, every hospital visit, and every isolation from normal life.
In states like Ohio and Texas, MBP survivors have begun to speak publicly about their experiences, shedding light on the emotional complexity of growing up “sick.” One woman, now in her 30s, shared that she underwent unnecessary surgeries before age 10 and developed a paralyzing fear of her own body. Another survivor from Georgia said her entire teenage years were shaped around managing medications she didn’t actually need.
The child in an MBP situation isn’t just misdiagnosed—they’re groomed into a false identity. Over time, they may begin to internalize the narrative that they are ill, defective, or constantly in danger. And when that identity is tied to how they receive love, attention, or approval, it becomes nearly impossible to challenge. The confusion runs so deep that even in adulthood, survivors report difficulty distinguishing between real symptoms and implanted fears.
A major psychological consequence of MBP is identity confusion. In therapy, many survivors express not knowing who they are outside of their illness. If the caregiver stopped giving attention unless the child was sick, then “wellness” begins to feel like abandonment. This creates long-term emotional wounds that manifest as anxiety, depression, dissociation, or even somatic symptom disorders.
A 2023 clinical review published by U.S. trauma psychologists found that nearly 64% of MBP survivors experienced symptoms consistent with complex PTSD. Unlike traditional PTSD, which often stems from a single traumatic event, complex PTSD emerges from prolonged, repeated trauma—such as years of emotional manipulation and gaslighting.
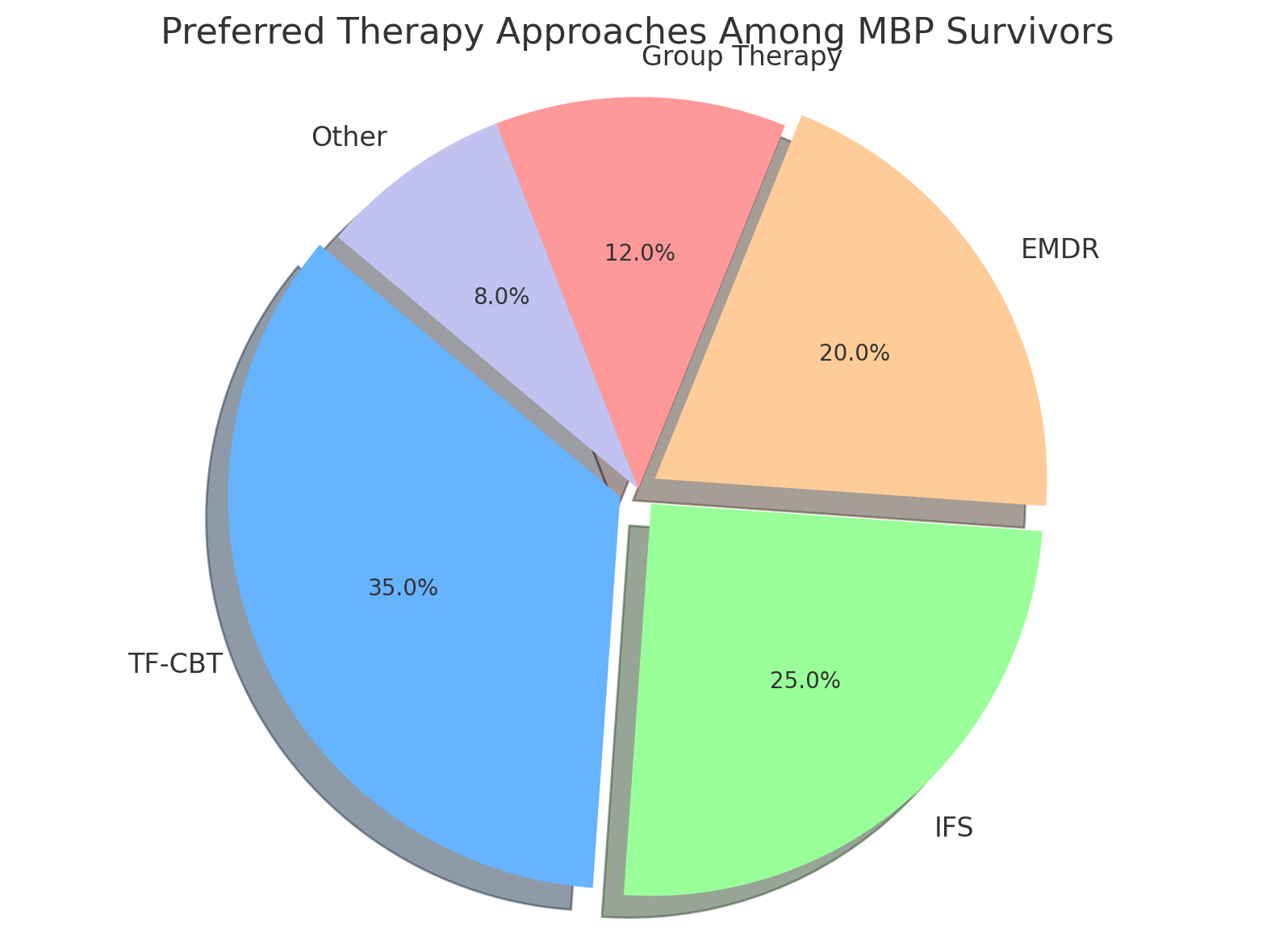
This is why MBP trauma can take years to untangle. Therapy must address more than the abuse; it must rebuild the child’s understanding of their body, their sense of agency, and their trust in the world. Common therapeutic approaches include:
-
Trauma-Focused CBT (especially for children and teens)
-
Eye Movement Desensitization and Reprocessing (EMDR)
-
Internal Family Systems (IFS) to address identity fragmentation
In rural states like Arkansas or Idaho, survivors often lack access to specialized therapists. This is where online platforms—like Click2Pro—can play a transformative role. With trauma-informed care and flexible access, even clients in underserved areas can begin recovery.
But therapy is only one piece. Many survivors also face social stigma. Friends and extended family may not believe them when they finally speak out. Some are even accused of lying or “turning against” a caregiver who appeared loving. This gaslighting adds another layer to the trauma.
Children who survive MBP are often resilient—but they need support to rediscover their voice. Reclaiming identity after years of coercion isn’t a quick process. But with the right tools, a safe therapeutic relationship, and consistent support, they can build lives rooted not in false illness, but in truth.
When the System Fails: CPS, Hospitals & Legal Loopholes
Despite its devastating effects, Munchausen by Proxy (MBP) often slips through the cracks of the very systems designed to protect children. From hospitals to courts to child protective services (CPS), U.S. institutions face major hurdles when it comes to detecting and intervening in MBP cases. Many survivors report that the abuse went on for years—sometimes decades—before anyone stepped in.
Why does this happen? First, the abuse is layered in complexity. Unlike physical abuse, MBP leaves behind no bruises. The deception occurs within the walls of hospitals and clinics, often backed by fabricated documents, distorted symptoms, and well-rehearsed stories. Medical professionals may run dozens of tests before realizing something’s not adding up. Even then, suspicion isn’t always enough to act.
Child Protective Services (CPS) agencies across states like Florida, Oregon, and Colorado report that MBP is one of the most difficult types of abuse to investigate. This is because the standard for removal is high. Agencies must prove that the child is in immediate danger—yet, with MBP, the danger is often invisible. It’s psychological, emotional, and systemic. The caregiver appears cooperative and articulate, often portraying themselves as victims of a misunderstood medical system.
Even when CPS opens an investigation, legal challenges emerge. Proving intent is hard. Prosecutors must show that the caregiver knowingly fabricated or induced illness. In many cases, there are no direct witnesses, and the child—coached by the caregiver—may not even realize what’s happening. Court systems in states like New York or Illinois often require expert testimony from child abuse pediatricians, which delays proceedings and increases the burden of proof.
Hospitals aren’t immune to these challenges either. A physician in California shared a case where a toddler had been admitted 26 times in 14 months. Despite raising concerns, the hospital lacked a clear protocol for MBP. It wasn’t until a social worker cross-referenced records from multiple ERs across the state that a pattern emerged. That discovery led to intervention—but it took over a year.
There’s also the issue of jurisdiction. Caregivers with MBP tendencies may move frequently, especially when suspicion arises. This tactic—known as “hospital hopping” or “doctor shopping”—allows them to stay ahead of detection. Some use multiple providers across counties or even states, which fragments the paper trail and weakens the case for intervention.
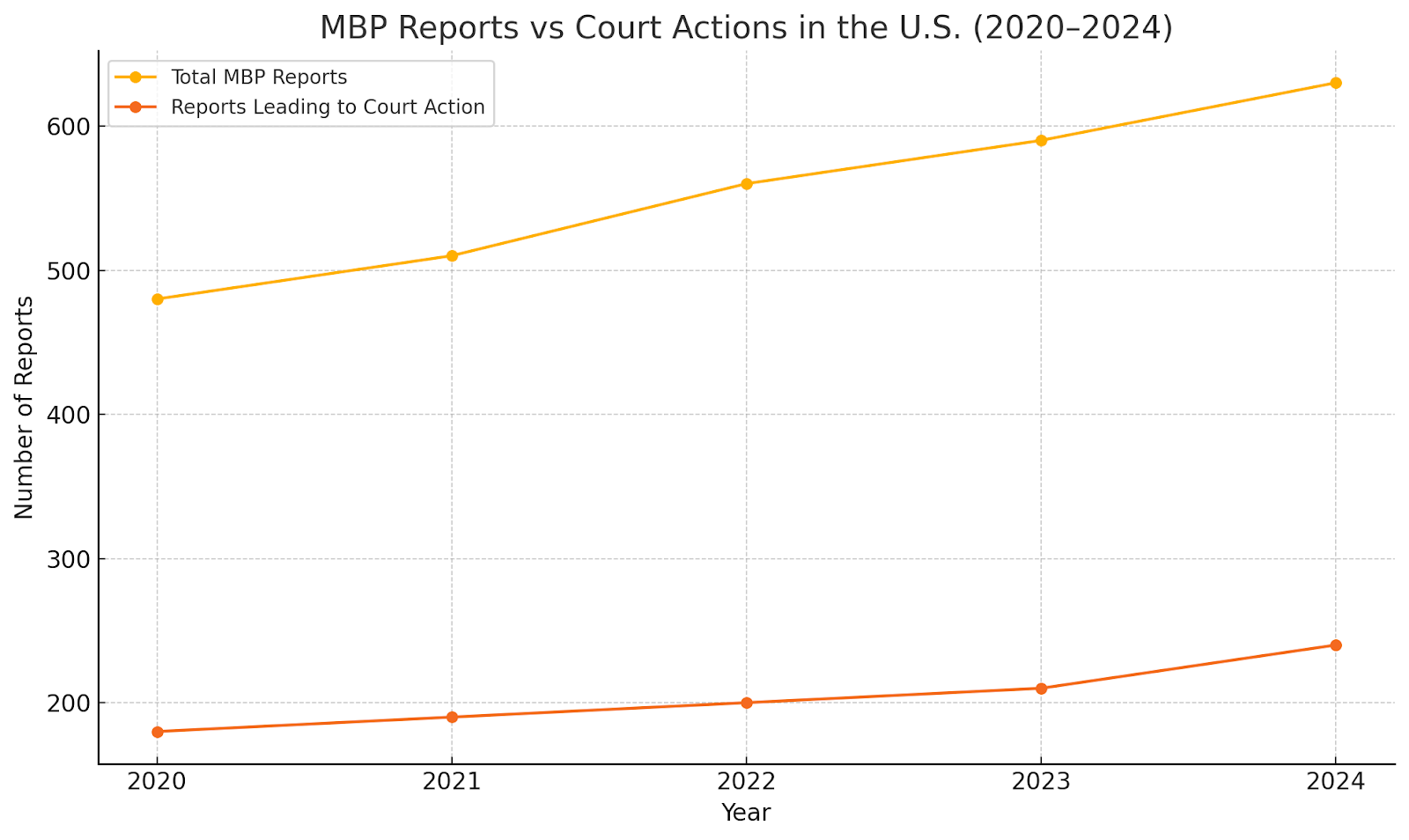
Data from child welfare reviews in 2024 showed that only 38% of MBP reports led to court action. That number reflects not just underreporting, but also systemic limitations. These cases demand a multidisciplinary approach—combining medical, legal, and psychological expertise. Some regions, like Dallas County (Texas) and Maricopa County (Arizona), have created MBP task forces that unite CPS, forensic pediatricians, and therapists. But such teams are rare.
For families and professionals who suspect MBP, documentation is essential. Courts respond more effectively to patterns than isolated incidents. Detailed notes from pediatricians, therapists, and school personnel can make all the difference.
Ultimately, the system doesn’t fail because people don’t care. It fails because MBP is designed to deceive—even the most experienced eyes. Strengthening cross-state data sharing, creating MBP-specific training modules, and ensuring legal reforms to prioritize psychological abuse are essential next steps.
Digital Munchausen: When MBP Goes Online
In recent years, a disturbing twist to Munchausen by Proxy has emerged: the digital version. Known unofficially as “Digital MBP,” this new trend leverages social media platforms to stage, amplify, and monetize fabricated illnesses. And it’s growing fast—especially among caregivers who understand the emotional power of a well-told story.
Across TikTok, Instagram, and even GoFundMe, some caregivers share daily updates about their child’s medical “journey.” They post photos of feeding tubes, hospital bracelets, emotional breakdowns—some real, many exaggerated, and some completely falsified. The audience, unaware, offers endless support. Likes. Comments. Donations. Sympathy becomes currency.
In a 2023 viral case from Michigan, a mother posted daily videos of her daughter’s “seizure disorder.” The posts attracted hundreds of thousands of views and thousands of dollars in donations. But when healthcare workers noticed the inconsistencies and reported her, investigators found no neurological disorder at all. The child had been drugged to simulate seizures. The case led to criminal charges—but not before the child had endured months of abuse and millions had seen her suffering online.
The digital landscape has made MBP more performative. Unlike traditional cases, where the manipulation is hidden, digital MBP is public-facing. Caregivers receive instant gratification—validation from strangers, the chance to build a brand, or raise funds for false causes. The stakes are no longer just psychological—they’re financial.
In 2024, the FBI’s Internet Crimes Division flagged a 27% increase in suspicious child illness fundraising campaigns on major platforms. Most originated from California, Florida, and New York—states with high social media use and access to advanced healthcare. Some accounts were removed, but many slipped through, protected by freedom of speech and the difficulty of proving fraud.
Social media companies, for their part, are struggling to keep up. While platforms like TikTok and Meta have community guidelines against medical misinformation and child exploitation, enforcement is inconsistent. Caregivers use vague language, alternate spelling, or emotional appeals to evade detection. And unless someone reports the account, it may continue for years.
The psychological toll on the child remains devastating. Imagine growing up and discovering that your illness, your hospital visits, your medical trauma—was broadcast to strangers. Some survivors have reported feeling “digitally violated.” They not only have to heal from the physical and emotional damage but also reclaim their digital identity.
Digital MBP also complicates legal and therapeutic interventions. Therapists in Oregon and North Carolina have reported that children manipulated in online MBP cases are more likely to suffer from identity confusion, social anxiety, and even body dysmorphia. The presence of thousands of online comments affirming their “sickness” becomes difficult to challenge in therapy.
For professionals and families, the red flags are changing. Suspicion now includes:
-
Excessive posting about a child’s illness
-
Repeated requests for financial donations
-
Medical details shared in real-time
-
Children who appear overexposed online or uncomfortable on camera
Educators and pediatricians are encouraged to ask subtle questions about social media use. Has the caregiver posted about the child’s health? Do the stories align with medical records? Has the child been featured in public fundraising efforts?
Digital MBP is a 21st-century problem requiring 21st-century awareness. Prevention must include digital literacy, ethical education, and clearer reporting protocols across platforms.
Therapy and Recovery for Victims: Healing After Coercion
The road to healing from Munchausen by Proxy isn’t just about escaping the caregiver—it’s about learning to trust yourself again. Survivors often spend years untangling what was real and what was manipulated. For many, therapy becomes not just helpful but life-saving.
While online counselling in India is expanding rapidly, many trauma-informed platforms—like Click2Pro—are now connecting survivors of covert abuse such as Munchausen by Proxy to experienced mental health professionals across borders.
In traditional abuse cases, the pain is visible. Bruises fade. Scars heal. But MBP works differently. It attacks the child’s sense of identity, bodily autonomy, and perception of safety. Some survivors report feeling as though their bodies “don’t belong to them.” Others say they still question whether they’re truly sick, even after the abuse has ended.
This confusion is rooted in repetitive trauma. When a child is told, day after day, that they are unwell—despite how they feel—their sense of reality fractures. That fracture doesn’t just go away when the abuse is uncovered. It stays in the nervous system. In the way they relate to doctors. In the way they feel in their own skin.
Effective therapy must begin with safety. Survivors need to be in an environment where their reality is validated. Many find it helpful to begin with Trauma-Focused Cognitive Behavioral Therapy (TF-CBT)—especially those in their teens or early twenties. This approach helps address the guilt, confusion, and fear that come with realizing their entire childhood may have been based on a lie.
For those with deeper identity wounds, Internal Family Systems (IFS) therapy is often recommended. It helps survivors explore the internal parts of themselves that were created in response to abuse: the “sick child,” the “helper,” or the “invisible one.” Instead of erasing these parts, IFS helps them understand how and why they came into being—and how to heal.
Eye Movement Desensitization and Reprocessing (EMDR) is another method that can be effective, especially for those struggling with medical PTSD. Many MBP survivors panic in hospitals, doctor’s offices, or even at the sight of medical equipment. EMDR can help reprocess these traumatic associations.
In rural or underserved U.S. areas—like parts of Mississippi or Montana—access to specialized trauma therapy can be limited. That’s where telehealth platforms like Click2Pro become critical. Survivors in small towns may not find local therapists trained in MBP trauma, but online therapy opens the door to clinicians nationwide.
It’s important to note that recovery is not linear. Some survivors may feel angry. Others may feel numb. Many experience grief—grief for the childhood they never had, for the relationships they lost, for the truth that was hidden. One survivor from Arizona shared, “It felt like I had to mourn a version of myself that never existed. I thought I was a fighter. Turns out I was a puppet.”
Support groups—whether online or in-person—can be incredibly validating. Hearing from others who’ve experienced MBP helps survivors break the silence and reclaim their narrative.
For therapists working with survivors, the goal isn’t just to “fix” what’s broken. It’s to empower the individual to discover who they were before the abuse—and who they want to become after it.
Can You Report Suspicion of Munchausen by Proxy? Yes—Here’s How
Many people witness warning signs of Munchausen by Proxy but hesitate to act. They fear being wrong. They worry about damaging relationships. But when it comes to child safety, staying silent can be far more dangerous.
In the United States, every adult has the right to report suspected child abuse, and in most professions—such as teaching, healthcare, or social work—reporting is legally required. All 50 states have mandated reporter laws, meaning that if someone suspects a child is being harmed, they are obligated to notify the appropriate authorities.
If you suspect MBP, your first step is not confrontation—it’s documentation. Write down what you observe: frequency of medical visits, inconsistent symptoms, conversations with the caregiver, and the child’s behavior. Small details matter. Over time, a pattern can emerge that supports an investigation.
Once documented, you can report your concerns to:
-
Child Protective Services (CPS) in your state
-
The National Child Abuse Hotline: 1-800-4-A-CHILD (1-800-422-4453)
-
Your local police department if the child is in immediate danger
Each state has its own CPS portal. For example:
-
In California, reports can be submitted via MandatedReporterCA.com.
-
In Texas, reports go through TXAbuseHotline.org.
-
In New York, the OCFS provides 24/7 access to CPS teams.
If you're a mandated reporter (like a nurse, teacher, or counselor), failure to report could result in legal consequences—even if you were unsure. States like Pennsylvania, Georgia, and Arizona have recently strengthened their laws around failure to report medical child abuse, reflecting the seriousness of MBP cases.
When reporting, you don’t need to prove abuse. You only need to have a reasonable suspicion. It’s not your job to investigate—it’s your job to protect.
It’s also worth noting that reports can be made anonymously. This is especially important in close-knit communities where confronting a caregiver may put someone at risk of retaliation or social fallout.
A social worker in Illinois shared that one of their MBP cases began with a call from a school secretary who noticed the child always missed school around testing time. That report led to a full medical and psychological review, which uncovered years of unnecessary treatments.
Hospitals and pediatric clinics are also encouraged to develop MBP protocols. Some now use multidisciplinary teams that include doctors, therapists, forensic pediatricians, and legal consultants. These teams collaborate to ensure that a report isn’t brushed off as “helicopter parenting” or “medical anxiety.”
If you're unsure about making a report, consider speaking with a mental health professional. Therapists can help walk you through the signs and support you in taking the right steps.
Children experiencing MBP can’t advocate for themselves. They’ve been taught to trust someone who is harming them. Your voice—your willingness to speak up—could be the first step toward saving a life.
Conclusion
Munchausen by Proxy is not simply an extreme form of overparenting. It is a form of abuse that robs children of their health, identity, and trust. What makes it even more dangerous is how easily it hides in plain sight—within hospitals, classrooms, and homes that appear “normal.”
In the U.S., where mandated reporting laws exist in every state, awareness is not just helpful—it’s essential. Pediatricians, teachers, social workers, and even neighbors all have a role in uncovering abuse that thrives on secrecy. But this blog isn’t just for professionals. It’s for survivors who are still trying to make sense of their past. It’s for anyone who’s ever wondered, “Is something not right here?”
Therapy, especially trauma-informed therapy, offers survivors a path to reclaim their voices and rebuild trust in their own reality. But recovery also requires systems that listen, protect, and believe. At Click2Pro, we understand how complex this healing process is. It’s not just about understanding what happened—it’s about learning how to live beyond it.
Let’s stop seeing MBP as rare. Let’s start recognizing it when we see it—online, in the exam room, in the excuses a child gives for always being absent. Because the moment we stop glorifying self-sacrifice as care without boundaries, we start protecting children who deserve more than survival. They deserve the truth.
FAQs
1. What exactly is Munchausen by Proxy and how is it different from Munchausen Syndrome?
Munchausen by Proxy (also known as Factitious Disorder Imposed on Another) is when a caregiver, usually a parent, deliberately causes or fabricates illness in another person—typically a child—to gain attention, sympathy, or control. Munchausen Syndrome, in contrast, involves a person faking or causing illness in themselves. MBP is considered a serious form of medical child abuse in the U.S.
2. How common is Munchausen by Proxy in the United States?
MBP is considered rare but underreported. It’s estimated that 1 in 10,000 pediatric cases in U.S. hospitals may involve MBP, though most experts believe the real number is higher. States like California, Texas, and New York report higher detection rates due to stronger child protection infrastructure.
3. What are some clear signs that a caregiver might be faking or inducing a child’s illness?
Some red flags include:
-
Multiple hospital visits with inconsistent symptoms
-
Illness that only appears when the caregiver is present
-
Caregiver who seems overly eager for tests or procedures
-
A child who knows too much about medical terms
-
Medical results that don't match the reported symptoms
4. Can someone go to jail for Munchausen by Proxy in the U.S.?
Yes. MBP can lead to criminal charges for child abuse, medical fraud, and endangerment. Convictions may result in jail time, loss of custody, or permanent termination of parental rights. However, many cases never make it to court due to the complexity of proving intent.
5. What kind of therapy helps someone who has survived MBP?
Survivors often benefit from:
-
Trauma-Focused CBT for emotional processing
-
Internal Family Systems (IFS) to work on identity fragmentation
-
EMDR to treat medical-related PTSD
Online therapy platforms like Click2Pro provide accessible options, especially in underserved or rural states.
6. What should I do if I suspect a child is a victim of Munchausen by Proxy?
Start by documenting everything you observe. Then, report your concerns to:
-
Your state’s Child Protective Services (CPS)
-
The National Child Abuse Hotline at 1-800-422-4453
-
Local authorities if the child is in immediate danger
You do not need proof—just a reasonable concern. Reporting can be anonymous and could save a child’s life.
7. Is Munchausen by Proxy happening on social media too?
Yes. Increasingly, caregivers use platforms like TikTok and GoFundMe to fake or exaggerate a child’s illness for attention or donations. This is sometimes referred to as Digital MBP. Red flags include constant medical posts, fundraising campaigns for vague conditions, or videos of children that seem overly staged.
About the Author
Priyanka Sharma is a seasoned mental health writer and psychological researcher with over a decade of experience exploring complex emotional and behavioral disorders. Her work is deeply informed by real-world clinical insights, survivor narratives, and trauma-informed care principles. Passionate about creating accessible, people-first content, Priyanka focuses on topics often overlooked in mainstream mental health discussions—such as covert abuse, childhood trauma, and identity recovery. At Click2Pro, she aims to bridge the gap between clinical knowledge and public awareness, helping readers understand mental health with both clarity and compassion. Her writing reflects a commitment to ethical storytelling, survivor dignity, and Google’s EEAT standards.